One afternoon in July, deep within the labyrinthine halls of the Medical Sciences Building at UC San Francisco’s hilltop campus on Parnassus Avenue, the laboratory of Alex Marson, MD, PhD, is buzzing. Doors clap. Gloves snap. Keyboards clack. Cells incubate in nutrient baths the color of Kool-Aid while machines resembling rice cookers spin mixtures of molecules, separating large from small. Every now and then, a printer whirs with notes for a new experiment, like a lunch order arriving in a restaurant kitchen.
Theo Roth, an MD-PhD student, opens a deep freezer, releasing an icy cloud. Here, amid frosted boxes stacked on frosted shelves, is the impetus for all this activity – the reason Roth and Marson and their colleagues at UCSF and elsewhere have begun to suspect, with no small amount of excitement, that they are in the vanguard of a new era in medicine.
Roth pulls out a box and lifts from it a transparent plastic vial no taller than a toothpaste cap. Inside, he explains, are billions of intricately folded, ribbon-like molecules: proteins known as Cas9. When linked to other molecules called guide RNAs, the Cas9 proteins transform into …
“… the magic CRISPR system,” Roth says, holding the vial up to the light.
Its contents look like … well, nothing. “Just another clear liquid,” Roth jests – because as he well knows, these molecules’ humble appearance belies a singular and extraordinary power.
The coming CRISPR cures
If you’ve heard of CRISPR (pronounced “crisper”), a hot topic in science circles nowadays, you’ve likely encountered a dizzying array of definitions and divinations. Is CRISPR a therapy? A revolution? A pair of genetic scissors? A text editor? A genesis engine? A gateway to designer babies? And what does that catchy acronym – which stands for “clustered regularly interspaced short palindromic repeats” – even mean?
Put simply, CRISPR is a tool. In fact, it is many tools – more precisely described as CRISPR systems – exquisitely engineered for operating on life’s tiniest anatomy: DNA, the substance of genes. These tools aren’t the first of their kind, but they are by far the most exacting, the cheapest, and the easiest to use. Dispatched into living cells, they can be made to manipulate any gene in any tissue in any organism, whether microbe, mouse, or monkey.
Or human. Just six years after the discovery of CRISPR technology, hundreds of research labs around the world are now using it to study patients’ cells and to create animal models of human diseases – from common illnesses to inherited disorders so rare that they may affect only a few families. This fast-growing body of research has proven a boon to medical science, showing how DNA – a spiraling chain of chemical bases strung together like rungs on a ladder – keeps us alive and healthy, and how even subtle changes in this code can make us sick.
But for physician-scientists like Marson and young trainees like Roth, the ascendancy of CRISPR systems raises an even grander hope: If these tools can illuminate the causes of disease in the laboratory, why not bring them into the clinic to treat patients?
What CRISPR scientists envision – the future they are now preparing for – is a whole new field of medicine. They even have a name for this nascent specialty: genome surgery. Just as today’s surgeons use steel instruments to excise tumors, repair blood vessels, or transplant kidneys, tomorrow’s genome surgeons could use CRISPR systems to remove one faulty gene, correct another, or replace a third – thereby curing genetic diseases at their source.
“Imagine a world where people go to the doctor, and they get their genome sequenced and learn they have a genetic disorder,” says Jennifer Doudna, PhD, who famously pioneered the first CRISPR applications in 2012. “And instead of telling them they need to live with that disorder, we have the technology that can actually treat them – potentially even cure them.”
It’s a lofty vision but one that may be within reach. In 2014, Doudna – who is a professor of chemistry and of molecular and cell biology at UC Berkeley and a senior investigator at the Gladstone Institutes, an independent research institute affiliated with UCSF – helped found the Innovative Genomics Institute (IGI), a partnership between UCSF and UC Berkeley to apply CRISPR systems to improving human health. (Its mission later expanded to also encompass food security and environmental sustainability.) Since then, teams of researchers and clinicians in the Bay Area alone – many of them funded through the IGI – have begun to work toward new CRISPR surgeries that could treat an array of diseases, including genetic disorders of the eye, nerves, kidneys, blood, and immune system.
“The possibilities are mind-boggling,” says Marson, an associate professor of microbiology and immunology and the scientific director of biomedicine at the IGI. He, together with Roth and others, is developing CRISPR-based techniques aimed at reprogramming patients’ own immune cells to kill cancer and to ward off HIV. The day when treatments like these enter the clinic may not be so far off.
Publications about CRISPR
In 2012: 139
In 2017: 3,080
Source: PubMed
Rare Genetic Diseases
Known: 6,259
Curable: 0
Source: Online Mendelian
Inheritance in Man
What CRISPR scientists envision – the future they are now preparing for – is a whole new field of medicine. They even have a name for this nascent specialty: genome surgery. Just as today’s surgeons use steel instruments to excise tumors, repair blood vessels, or transplant kidneys, tomorrow’s genome surgeons could use CRISPR systems to remove one faulty gene, correct another, or replace a third – thereby curing genetic diseases at their source.
“Imagine a world where people go to the doctor, and they get their genome sequenced and learn they have a genetic disorder,” says Jennifer Doudna, PhD, who famously pioneered the first CRISPR applications in 2012. “And instead of telling them they need to live with that disorder, we have the technology that can actually treat them – potentially even cure them.”
It’s a lofty vision but one that may be within reach. In 2014, Doudna – who is a professor of chemistry and of molecular and cell biology at UC Berkeley and a senior investigator at the Gladstone Institutes, an independent research institute affiliated with UCSF – helped found the Innovative Genomics Institute (IGI), a partnership between UCSF and UC Berkeley to apply CRISPR systems to improving human health. (Its mission later expanded to also encompass food security and environmental sustainability.) Since then, teams of researchers and clinicians in the Bay Area alone – many of them funded through the IGI – have begun to work toward new CRISPR surgeries that could treat an array of diseases, including genetic disorders of the eye, nerves, kidneys, blood, and immune system.
San Francisco Area Genome Surgery Projects
CRISPR-based surgeries currently in development at UCSF, UC Berkeley, the Gladstone Institutes, and the Innovative Genomics Institute aim to treat the following conditions:
Sickle Cell Disease (a blood disorder)
Best Disease (an eye disorder)
Charcot-Marie-Tooth (a neurodegenerative disorder)
Severe Combined Immunodeficiency
Cancer
HIV Infection
Autoimmune Disorders
Polycystic Kidney Disease
Obesity
Hemophilia (a blood disorder)
“The possibilities are mind-boggling,” says Marson, an associate professor of microbiology and immunology and the scientific director of biomedicine at the IGI. He, together with Roth and others, is developing CRISPR-based techniques aimed at reprogramming patients’ own immune cells to kill cancer and to ward off HIV. The day when treatments like these enter the clinic may not be so far off.
Imagine a world where, instead of telling people they need to live with a genetic disorder, we have the technology that can actually treat them – potentially even cure them.”
Jennifer Doudna, PhD
New hope for rare disorders
While Marson’s team busies itself remodeling immune cells, a few miles away at the Gladstone Institutes, on UCSF’s Mission Bay campus, a different sort of genome surgery is underway. There, in the laboratory of senior investigator Bruce Conklin, MD – a UCSF professor of medicine and IGI’s deputy director – the cells of 19-year-old Delaney Van Riper are undergoing experimental procedures that could one day cure her of a worsening disability.
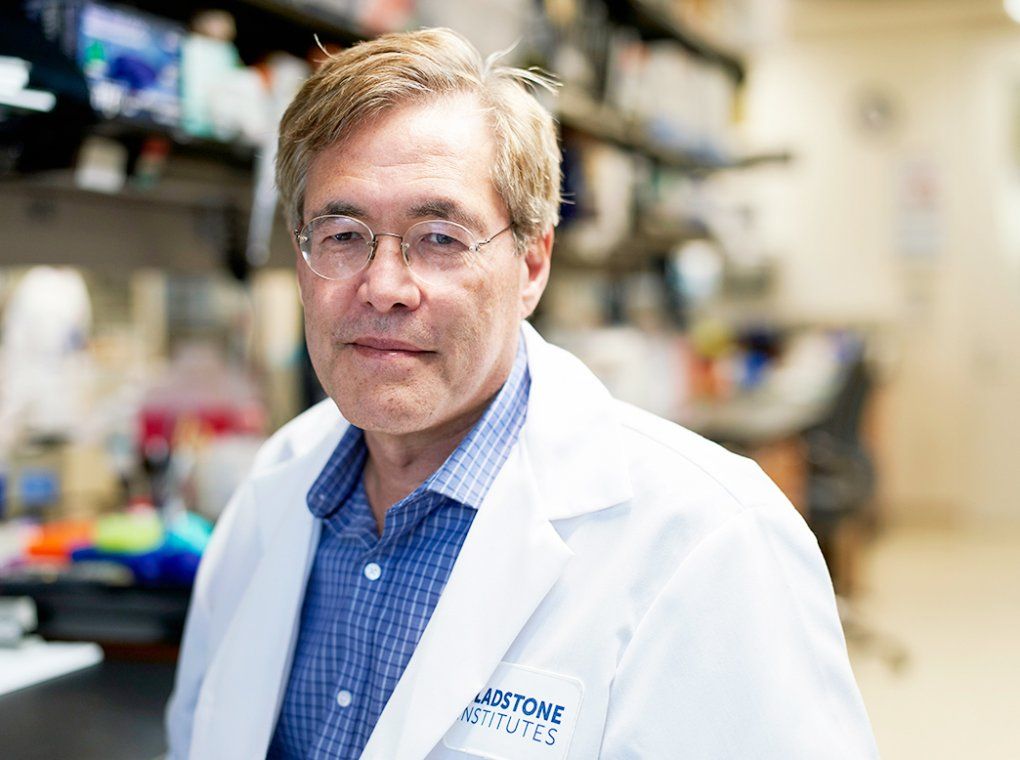
Bruce Conklin, MD, is exploring how CRISPR technology could treat genetic diseases. Photo: Steve Babuljak
Van Riper was born with a rare disease called Charcot-Marie-Tooth (CMT), one of more than 6,000 known genetic disorders, which arise from specific variations in DNA. Such variations – called mutations – throw a wrench in a cell’s protein production line, thus creating deviant or defunct molecules, like Ikea furniture assembled from garbled instructions. In some cases, a mutation in just one DNA base – out of the total 3 billion pairs of bases in the human genome – can wreak severe havoc.
Van Riper’s mutation produces a miscreant protein that degrades her nerve cells’ ability to relay messages between her brain and her muscles, causing her to slowly lose control of her limbs. She was diagnosed at age 7, after her father, a genetic counselor, noticed that she wasn’t walking normally. By age 8, she wore leg braces, laughing along with the kids who called her Forrest Gump, “so they didn’t see me as a cripple.” By age 13, she struggled to hold a pencil.
“There are certain muscles I just don’t have anymore,” she says during a recent visit to the lab. She is seated at a conference table, where a dozen or so researchers from Conklin’s group have gathered to meet her, many of them for the first time.
The researchers know her cells intimately, however. They have isolated them from samples of her blood and nurtured them in petri dishes. They have doused these blood cells with a cocktail of genes that turns them into stem cells, undifferentiated cells that can grow indefinitely. Using another gene cocktail, they have coaxed the stem cells to become nerve cells like those at the root of Van Riper’s disease. They have examined these diseased nerve cells through microscopes, studied their troublesome mutation, and sent in CRISPR systems to try to remove it.
All the while, Conklin and his team have dreamed about a day when a physician might inject CRISPR molecules directly into Van Riper’s spine to heal the nerve cells there; a day when the success of this pilot surgery will lead to more CRISPR operations for more diseases; a day when patients who once had no hope will come to San Francisco from all over the world to seek these treatments out.
Delaney Van Riper (left) was born with a rare disease called Charcot-Marie-Tooth (CMT), and had donated cells to the lab of Bruce Conklin, MD (right), so he can test DNA surgeries that aim to cure people like her who have rare genetic disorders. Photo: Steve Babuljak
Now the researchers want to know all about this dark-haired teen who wears black skinny jeans, Converse sneakers, and a lip-ring; who has trouble using her hands and sometimes stumbles over her feet but sits with exquisite posture; who speaks eloquently and vulnerably about the disease that once made her question who she is and inspired her to become a writer and a medical trailblazer.
“How does it feel to be part of this project?” someone asks.
“It’s nice to realize people are looking into a solution for people like me who don’t have any solutions,” Van Riper says. “I feel you really care.” She flashes a grin and adds, “I like nerds.”
“Do you worry about the risks?”
“I’ve lived long enough to have an experience of life with a disability. If something goes wrong, I don’t think it would be as scary as some people think. We can’t know until we do it. I’m fine being that person doing it.”
“You’re really brave.”
“I know it’s not a for-sure fix. Secretly, though, I do think it will work.”
So do many of Conklin’s patient volunteers. Some, like Van Riper, have CMT; others have genetic mutations that cause BEST disease, an eye disorder that leads to blindness.
It’s nice to realize people are looking into a solution for people like me who don’t have any solutions. I feel you really care.”
Delaney Van Riper
Conklin’s team is starting with these two rare diseases for several reasons. First, they each arise from well-known mutations in a single gene, making the CRISPR surgeries relatively simple to design. Second, they affect tissues where CRISPR systems can be easily administered and their effects easily measured. Third – and perhaps most important – these diseases are currently untreatable; any relief from their devastation is, for most patients, worth the potential risks (which may include, for instance, cuts in undesired parts of the genome).
“Almost universally, the first targets of genome surgery will be incurable diseases, where there is truly no other option,” Conklin says. “If we can treat these, it will open the door to a new type of medicine.”
An unexpected windfall
It’s easy to see, even for the researchers involved, how the promise of genome surgery can sound like magic. Of course, the process is not magic at all but a very real, albeit exceptional, molecular operation that traces its origin to an unassuming source.
Starting in the 1980s, biologists studying bacteria and other microorganisms noticed strange regions of DNA in their genomes. Surprisingly, the regions contained segments that were palindromes – they read the same forward as backward – and that repeated at regular intervals, like books in which every paragraph begins with the word “RACECAR.” Those oddities gave the segments their mouthful of a name: clustered regularly interspaced short palindromic repeats, soon shortened to CRISPRs.
Eventually, researchers determined that CRISPRs bookend pieces of DNA stolen from invading viruses, like frames around criminal mug shots. The whole DNA region serves as a kind of microbial defense force: Genes near the CRISPRs code for defender molecules, called CRISPR-associated (Cas) proteins, that execute viruses by chopping up their DNA; the viral mug shots, copied into RNA molecules that stick to the Cas proteins, serve as the defenders’ guides.
For decades, CRISPR research remained a relatively obscure niche of biology. Then, in 2012, a team led by UC Berkeley’s Doudna and Emmanuelle Charpentier, PhD, then of Sweden’s Umeå University and now a director at the Max Planck Institute for Infection Biology in Berlin, published a paper that launched CRISPR to scientific fame.
The paper described how one particular Cas protein, Cas9, could be directed to cut not only bacteria-invading viruses but any piece of DNA, simply by changing Cas9’s RNA guide. That ability – to create a specific DNA editor by supplying a specific RNA molecule – was revolutionary. RNA, after all, is easy to make in the lab. Scientists could therefore build a plethora of new Cas9-based tools in a fraction of the time and at a fraction of the cost of previous technologies. [See “Genome Editing Before CRISPR: A Brief History.”]
This discovery ignited a CRISPR frenzy. Around the world, labs quickly embraced the so-called CRISPR-Cas9 system, using it to cut out and splice genes into bacteria, fungi, plants, animals, and, of course, human cells. “It was just remarkable how fast it spread,” Doudna recalls. Soon, researchers were rejiggering Cas9 to create CRISPR tools with more diverse abilities, thus expanding Cas9’s scalpel into an array of surgical instruments.
In 2013, for instance, Doudna teamed up with several UCSF researchers – including Stanley Qi, PhD (now at Stanford University); Luke Gilbert, PhD (the Goldberg-Benioff Professor); Jonathan Weissman, PhD; and Wendell Lim, PhD – to show that a mutated version of Cas9, called “dead” Cas9, or dCas9, could bind to a DNA target but not cut it. This insight proved incredibly fruitful: By fusing various other molecules to dCas9, the team could use the resulting systems to dial up or dial down gene expression without altering the underlying DNA. “Now we had a volume switch,” says Weissman, a professor of cellular and molecular pharmacology and co-director of IGI.
Other labs soon found further add-ons: molecular tags to track genes’ behavior; molecular proofreaders to edit single bases; molecular shields to stop rogue cuts; molecular switches to allow remote control. “It was kind of amazing,” Weissman says. “In the course of just six years, we did everything we wanted and much more.”
The challenge now for genome surgeons is to find which combinations of CRISPR systems, in what order and under what conditions, will treat a particular patient with a particular disease safely and effectively.
On the Medical Frontier
Back in the Marson lab, Roth has mixed the ingredients for his “magic” CRISPR system in a flask and left them under heat to allow them to assemble. Now, using a syringe-like pipette, he sucks up the CRISPR molecules and divvies them, squirt by tiny squirt, among the wells of a honeycombed plate. There, he will test the system on human T cells — a type of immune cell — to see how well his surgical procedure works.
“In a clinical setting, this would be done by a robot,” he says, as if he’s already envisioning a day when all this tinkering — and tedious pipetting — will not only satisfy scientific curiosities but also save lives.
Learn how scientists are expanding their “CRISPR toolkit” by fusing various other molecules to dCas9, which dial up or dial down gene expression without altering the underlying DNA.
Next, he adds to the wells another ingredient: genes. These particular genes code for a protein called a synthetic T-cell receptor, or TCR. Perched on the surface of T cells like border guards, receptors detect toxic particles or pathogens entering the body, thereby instigating an immune attack. A synthetic TCR is a lab-made receptor designed specifically to recognize cancer cells – in this case, some forms of melanoma. If all goes as Roth expects, the CRISPR system will splice the TCR genes into the T cells’ DNA precisely where he wants them, turning the cells into cancer-killing agents. (In 2017, the U.S. Food and Drug Administration approved two older-generation T-cell therapies that use non-CRISPR technologies, one for acute lymphoblastic leukemia and the other for advanced lymphomas.)
“Genome surgery isn’t just about repairing DNA,” Roth says, now pipetting the human T-cells into the test wells to mingle with the CRISPR molecules and the TCR genes. “We also want to put new sequences into cells that impart new therapeutic functions.”
Finally, he slides the entire well plate – with its motley crew of residents – into a breadbox-sized contraption: an electroporator. Click, click, click goes the electroporator, delivering a series of mild electric shocks. The shocks make the T cells’ sack-like membranes permeable, letting the CRISPR molecules and the TCR genes slip through. When at last the electroporator ejects the cells, Roth sets them in an incubator to warm.

Theo Roth, an MD-PhD student, is developing CRISPR-based surgeries aimed at reprogramming patients’ own immune cells to treat cancer and HIV. Photo: Elena Zhukova
A couple of days later, after the CRISPR system has had time to perform its tricks, he will analyze the data. He will determine, to his satisfaction, that they are “somewhat as we expected.” Then he will start preparing the next experimental run – one of hundreds he has done over the past year and will continue to do in the months to come – in the hope of making the procedure just a little easier, a little safer, a little more effective.
Like most genome surgery pioneers, he is cautiously optimistic that his efforts will pay off. The rapid rise of CRISPR technology, followed by early therapeutic progress, has given scientists and physicians alike reason to be hopeful – to “feel encouraged,” as Doudna says, “that this is something that in the next few years will be increasingly available to patients.”
At the same time, many important questions remain: How will physicians deliver CRISPR systems to hard-to-reach tissues such as the heart? How will they treat diseases with many underlying and interacting gene mutations? How will they educate patients about the risks and benefits? What exactly are the risks and benefits? What are the proper doses? How will these surgeries be regulated? Who will perform them? Who will pay for them? Who will have access to them?
“There’s plenty of work still to be done,” Roth says, speaking for the field as well as himself. He and his peers are like Apollo engineers – tweaking one more sensor, running one more simulation – before launching a space flight, with astronauts aboard, into the starry unknown.
Even before liftoff, CRISPR therapies are already a pièce de résistance – a testimony to just how far science has taken us and where it yet may lead.